- European TFOS Ambassador Meeting - 2019
TFOS: Unmet needs and future solutions for ocular surface diseases in Europe
Jelle Vehof, M.D., Ph.D.
Section of Academic Ophthalmology, King's College London, London, UK, and Departments of Ophthalmology and Epidemiology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
Conflicts of Interest: The author has no conflicts of interest with regard to this report
Introduction
In response to a request from the Tear Film & Ocular Surface Society (TFOS), I have written this Executive Summary of the report entitled the "TFOS European Ambassador meeting: Unmet needs and future scientific and clinical solutions for ocular surface diseases." This report was recently published by multiple authors under the auspices of TFOS in The Ocular Surface,1 and this summary has been approved by the TOS Editor-in-Chief.
Executive Summary
In September 2019, 34 TFOS European ambassadors met to discuss the needs and challenges of ocular surface care in 25 European countries. The proceedings of that meeting were published in The Ocular Surface, and important information from that report is summarized in this presentation.
1
Europe comprises around 10 million square kilometers, which is about 7% of the earth’s land area. It has a relatively high population density, with 750 million inhabitants. It is considered a wealthy continent, but it has poorer regions, especially in the southern and eastern parts. There are also differences in cultural, political, climatic, and geographic aspects, and the health systems differ greatly between countries. For example, most countries have around 50-150 ophthalmologists per 1 million inhabitants (Figure 1). Greece is a positive outlier, and the United Kingdom, the Netherlands, and Ireland have relatively few
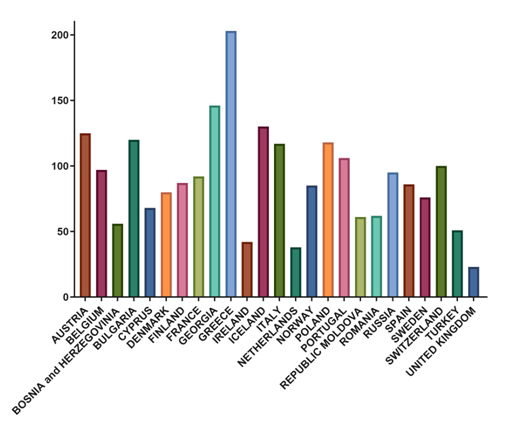
Figure 1. Number of ophthalmologists per 1 million inhabitants. Reprinted from Erickson S, et al. Ocul Surf. 2020.1
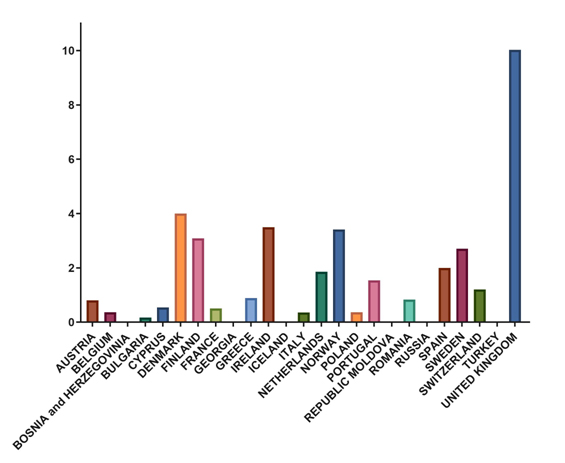
ophthalmologists. However, it is not only ophthalmologists that treat OSD. Figure 2 shows the number of optometrists per one ophthalmologist. Several countries have no optometrists at all, and some have only a few, while the United Kingdom has relatively few ophthalmologists and many optometrists. The same is true for the Scandinavian countries, the Netherlands, and Spain, but to a lesser extent.
One of the big challenges in eyecare in general in Europe is to provide timely care. There are long waiting lists across Europe to see an ophthalmologist, and sight-threatening disease is given first priority in most healthcare systems. OSD is regarded as a low priority. My Swiss colleague said, "More favorable clinical outcomes are likely achieved with earlier therapeutic intervention," and the Irish ambassador noted, "The greatest challenge we face is our inability to provide timely care. Long waiting lists hamper the delivery of care to patients with chronic OSDs like dry eye." Another problem is the limited time devoted to each patient visit, which is approximately 5-15 minutes for most ophthalmologist visits. This is not sufficient for the majority of OSDs. For example, DED requires several tests to establish a good diagnosis and treatment plan. The Spanish ambassador said, "More important, there is no time for discussion about the chronic nature of the disease and how to correctly use the various therapeutic options." Another problem is that there is limited interest in OSD as a sub-specialty among ophthalmologists. As noted by the Spanish ambassador, "Doctors are well trained, but are more interested in cataracts, DSAEK, and difficult glaucoma and retinal detachment cases than in DED." Similarly, the Turkish ambassador said, "We need to increase the awareness of DED and OSD, especially by young ophthalmologists, who are more focused on cataract surgery." This situation may be driven by financial reasons.
Several ambassadors stressed the need to provide OSD fellowships in their countries and more specialized training. The smaller countries especially stressed the need for international exchange programs to bring more knowledge into their countries. Some countries stressed the need for more tertiary referral OSD or corneal centers. For purposes of patient care and insurance coverage, there needs to be more awareness of DED as a serious disease affecting the quality of life of patients. As the Swedish ambassador said, "DED must be formally recognized as a medical condition." The Belgian ambassador said, "Dry eye is frequently considered more as a physiological condition than as a disease…and for the majority of my Belgian colleagues, DED is synonymous with Sjögren syndrome." These comments illustrate a problem existing in much of Europe. There also needs to be more awareness of recent advances in diagnostic and therapeutic options for DED. The Norwegian ambassador noted, "The main challenge is to increase ophthalmologists’ awareness of how DED can be diagnosed and treated… the risk of entering a vicious cycle of recurring disease is really under-appreciated."
Access to specialized eyecare could be increased by developing a greater role for optometrists. In addition to the variation in availability of optometrists among countries, there are major differences in their qualifications and expertise. For example, in the United Kingdom and Ireland, optometrists can have prescribing rights after extra training. They are well-trained, and they deal increasingly with even acute eye problems. In the Netherlands, guidelines are currently being developed to define which type of practitioner will treat which patients according to the stage of OSD. A greater role for optometrists could facilitate better care for OSD if patients can bypass waiting lists for ophthalmologists and have longer patient visits with optometrists. In Ireland, a nurse-led keratoconus diagnostic and crosslinking service in Dublin has been highly effective, but expansion of the program to other cities is hampered by a shortage of nurses.
A number of European ambassadors noted the need for more high-quality randomized clinical trials, particularly placebo-controlled, for the various new DED and MGD treatments, e.g., intense pulsed light or thermal pulsation systems. My Italian colleague commented on the scarcity of high-tech treatments in university and research settings compared to private practices. This problem exists in the Netherlands as well and is related to the lack of insurance coverage for these treatments in European public health systems. Conclusive studies that document the benefits of such treatments might make them eligible for insurance coverage.
More studies into personalized medicine are also needed. Which patient groups really benefit from personalized procedures, and what are the optimal treatment modalities? Other important research areas that were mentioned regarded the management of neuropathic ocular pain, and psychological aspects of DED. DED in the young is understudied. In the Netherlands, symptomatic DED is very prevalent in the younger adult age groups, with 20-30-year-olds having the highest prevalence. The use of electronic devices is potentially contributing to this problem, and more studies in this are needed. Surgical procedures are an important cause of DED, and prevention strategies should be studied and developed. The European ambassadors also noted the need for better biomarkers to diagnose inflammation at the ocular surface, as well as biomarkers to better differentiate between the different OSDs and possible sub-types of DED. Another biomarker might identify patients at risk of getting ocular graft versus host disease after allogeneic stem cell transplantation.
Options for management of OSDs are limited in Europe. There are increasing shortages of medications, particularly in countries that have set low drug prices, giving pharmaceutical companies little incentive to increase drug availability. Preservative-free glaucoma eye drops and topical acyclovir are unavailable or unaffordable in many areas. Ambassadors from Turkey and Bosnia and Herzegovina mentioned the need for better treatments for fungal ulcers and acanthamoeba keratitis. The number of non-preserved formulations is very limited in Russia and Bulgaria. In Poland, scleral lenses are rarely available. Many countries reported difficulties in obtaining cyclosporine or had problems with insurance coverage of cyclosporine, limiting optimal treatment of DED and allergic disease. Lacrimal punctal occlusion is not available in Russia. 'Soft steroids' or antivirals are unavailable in Moldova. Lissamine green is not available in Turkey. A lack of modern equipment due to financial limitations is a major problem in many countries, including Greece and Spain.
Some European countries have no tissue or organ banks. Several other countries reported difficulty in obtaining sufficient donor corneas or had a shortage of surgical centers that perform transplant procedures. For example, the Greek ambassador said that around 1,500 grafts a year were needed in Greece, but only 300 were performed. Most of them were performed during the annual American Academy of Ophthalmology meeting, as more donor material is available when US corneal surgeons are attending the meeting and not operating. Several countries reported major traumas from consumer fireworks, especially during New Year’s Eve or other holidays. Fireworks injuries are a big problem in the Netherlands, and although most of the public is against allowing the sale of fireworks, the government allows it.
In the larger countries, especially those with geographically remote areas, the distance a patient must travel to see an ophthalmologist hampers good treatment of OSD. Similarly, ophthalmologists working in remote areas find it difficult to travel to big cities to attend workshops and meetings for continuing education. Therefore, there is a need to create and distribute written educational materials.
In Italy, broad-spectrum topical antibiotics are over-prescribed for conjunctivitis -- not only bacterial conjunctivitis but all types of conjunctivitis. This is probably also true in many other countries, leading to the development of antimicrobial resistance in Europe. Turkey has many refugees entering the country from the Middle East and Africa, bringing trachoma and chicken pox, because they have lacked adequate healthcare. Bulgaria has an unusually high prevalence of corneal dystrophies, but there are no funds for genetic testing, hampering good diagnosis and treatment. Keratoconus is very common, but there is no contact lens-manufacturing laboratory locally, and contact lenses are imported from the UK. However, importing is increasingly difficult because of Brexit.
In summary, Europe is a diverse continent with varying needs and challenges in the management of OSD, mostly caused by financial, regulatory, and geographical differences. Many of the European ambassadors noted that OSD and particularly DED need to be recognized as serious diseases greatly affecting the quality of life of many people, even more than some sight-threatening diseases. Timely treatment is important, and practitioners need to be more aware of advances in diagnostic and therapeutic options. Optimal care of OSD is hampered by limited clinic time and long waiting lists to access care by ophthalmologists. A greater role for optometrists in the management of OSD could alleviate this problem, and several countries have taken successful initiatives in this regard. Finally, higher-level evidence studies are needed to assess newer management options in DED.
Reference
1. Erickson S, Sullivan AG, Barabino S, Begovic E, Benitez-Del-Castillo JM, Bonini S, et al. TFOS European Ambassador meeting: Unmet needs and future scientific and clinical solutions for ocular surface diseases. Ocul Surf. 2020 Oct;18(4):936-962. doi: 10.1016/j.jtos.2020.05.006. Epub 2020 Jun 3.



